Parkland Formula for Burns: Pediatric and Adult Examples
Parkland formula for burns made easy! Pediatric and adult calculator, examples, and practice questions! TBSA review using the Rule of Nines and more!
Save Time with a Video!
Save time by watching the video first, then supplement it with the lecture below!
Click below to view the EZmed video library. Subscribe to stay in the loop!
Parkland Formula for Burns
Welcome to the Parkland formula made easy!
The Parkland formula is used in burn patients to calculate the total amount of fluids to be given in the first 24 hours after injury.
The formula takes into account the patient’s body weight and total body surface area (TBSA) affected by the burn to determine the recommended fluid volume.
In this post, we will discuss the Parkland formula for both adults and pediatrics.
We will also review how to calculate TBSA using the Rule of Nines.
We will finish with an example and practice question, so make sure to read until the end!
Parkland Formula Calculator
As mentioned above, the Parkland formula can be used to calculate the initial fluid requirements in burn patients.
The Parkland formula for an adult is:
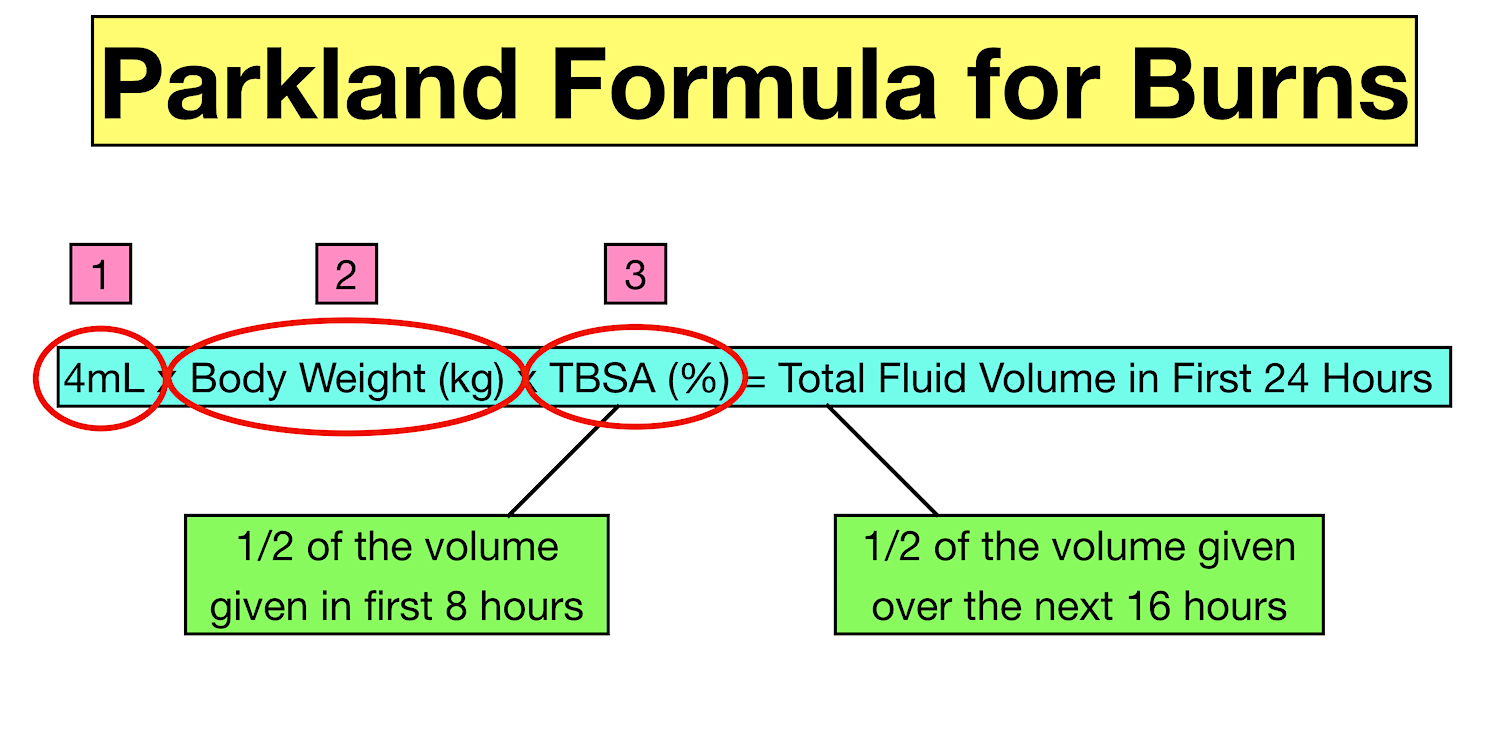
4mL x Body Weight (kg) x TBSA (%) = Total crystalloid fluids in first 24 hours
The equation will provide you with the estimated total amount of crystalloid fluids the patient should receive in the first 24 hours after a burn injury.
First 1/2 of fluids given in the first 8 hours
Second 1/2 of fluids given over the next 16 hours
Half of the total volume should be administered in the first 8 hours, and the other half should be administered over the next 16 hours.
IMPORTANT: The first 8 hours begins from the time of the burn injury, and not from the time of patient presentation, evaluation, or fluid calculation.
For example, if a patient presents to a hospital 2 hours after a burn injury, then they should receive the first half of their fluids within 6 hours instead of 8 hours.
This means the first half of their fluids may need to be administered at a faster rate.
Parkland Formula for Burns: Calculates the total amount of crystalloid fluid to be given in the first 24 hours after a burn injury
Parkland Formula Indications
The Parkland formula is used to estimate the extent of partial thickness and full thickness burns (2nd-degree burns and higher).
Superficial (1st-degree) burns are not included in the calculation.
The Parkland formula is typically used in burns involving > 20% TBSA for adults and > 10% TBSA in children or the elderly.
Burns involving a smaller TBSA typically do not generate a systemic inflammatory response and do not cause massive fluid shifts (more on that below!)
Furthermore, patient’s with smaller burns can usually tolerate fluids by mouth (PO).
Having said that, patient’s with smaller burns may still need IV fluids, and the Parkland formula still may need to be used on a case-by-case basis.
As the TBSA approaches 15-20% involvement, an inflammatory response is usually generated and IV fluid resuscitation using the Parkland formula is more likely.
The Parkland formula can also be used in those who have smaller burns but cannot tolerate PO fluids, such as injuries to the mouth or inhalation injuries.
Parkland Formula for Burns: Adult calculation and example indications for use
Parkland Formula TBSA
We can see the Parkland formula has 3 main variables:
4mL
Body Weight (kg)
Total Body Surface Area (%)
Parkland Formula for Burns: The equation includes 3 variable - (1) A constant; (2) Body weight in kilograms; (3) Total body surface area percentage
The first variable is 4mL, which is the constant for adults.
The easy way to remember “4mL” is to use the word “FOR” in “parkland FORmula”.
The second variable is the patient’s body weight in kilograms, which is also easy to calculate.
The final variable is the total body surface area (TBSA) involved by the burn.
This requires calculating.
IMPORTANT: Only the areas affected by partial thickness and full thickness burns (2nd-degree burns and higher) are counted toward the TBSA calculation.
Superficial (1st-degree) burns are not included in the calculation.
We will discuss 3 main methods for calculating TBSA below:
Rule of Nines
Lund and Browder Chart
Palmar Method
Rule of Nines
The Rule of Nines is one of the more common methods for calculating TBSA.
Check out the previous lecture on the Rule of Nines MADE EASY for simple explanations, colorful diagrams, and high-yield study guides with examples!
The Rule of Nines provides a body surface area (BSA) percentage for different body parts as shown in the table and diagram below.
The BSA percentages are mainly multiples of 9, which is how the rule gets its name.
These percentages can then be used in burn patients as a way to calculate the TBSA involved.
Parkland Formula TBSA: The Rule of Nines chart and diagram can be used to calculate the TBSA of a burn.
The Rule of Nines is fairly easy to remember and efficient to use.
The problem, however, is its accuracy in obese and pediatric patients.
While the Rule of Nines is useful in non-obese adults, it can be less accurate in children.
As mentioned in our Rule of Nines lecture, pediatric patients have disproportionately larger heads and shorter legs.
This can make the Rule of Nines less accurate as shown in the diagram and table below.
We can see the head is disproportionately larger at 21% instead of 9%, and the legs are disproportionately smaller at 13.5% each instead of 18% each.
Of note, the diagram and table are approximate percentages for infants and young children. These numbers can vary and will change in older pediatric patients.
The point is we can see how the Rule of Nines does not take into account variations in body shape with age.
This is where the Lund and Browder Chart comes into play.
Parkland Formula TBSA: The Rule of Nines is best for non-obese adults and is less accurate in a child, infant, or baby (pediatrics) due to body shape variations.
Lund and Browder Chart
The Lund and Browder Chart takes into account variations in body shape with age, and can be used in both adults and children to calculate TBSA.
We can see in the table below how the Lund and Browder Chart takes into account the size of the head and legs based on age.
The diagram shows the constant BSA percentages of the other body parts.
So you can see how the Lund and Browder chart can potentially provide a more accurate representation of the extent of the burn injury, especially in children.
The downside, however, is the Lund and Browder Chart is more challenging to remember and less efficient than the Rule of Nines.
Parkland Formula TBSA: The Lund and Browder Chart can be used to calculate the TBSA of a burn, and takes into account body shape variations with age
Palmar Method
The “rule of palm” or palmar method can also be used to estimate burn TBSA.
The method states:
The patient’s hand (including digits) = ~0.8-1% BSA
The patient’s palm (excluding digits) = ~0.5% BSA
This method is typically used in smaller burns.
IMPORTANT: Remember you are using the size of the patient’s own hand and not your hand to approximate the TBSA.
You may see mixed literature stating the palm alone is about 1% BSA.
However, this has recently been shown to be a potential overestimation and the palm is more accurately about 0.5% BSA.
Just be aware there can be accuracy issues with this method, and it is typically used in smaller burns.
Parkland Formula TBSA: The “rule of palm” or palmar method can be used to calculate the TBSA of a burn
Burn Shock - Fluid Resuscitation
Now that we know how to calculate TBSA, we can use the Parkland formula to determine the total volume of fluids to be given in the first 24 hours after injury.
Early fluid resuscitation is important, especially in severe burn patients.
In addition to causing local damage to the skin and tissue, severe burns can generate a systemic inflammatory response which can affect the entire body.
Capillary permeability increases during an inflammatory response, and intravascular fluid can leak into the interstitial space.
In other words, fluids within blood vessels leak into spaces outside the vasculature where it does not belong.
The capillary leak can result in large fluid shifts from the intravascular to the interstitial space, which can cause intravascular volume depletion and edema.
Parkland Formula Fluid Resuscitation: Severe burns can generate a systemic inflammatory response and increase capillary permeability. This can lead to fluid shifts, intravascular hypovolemia, and edema.
Burn Shock
The intravascular hypovolemia (volume depletion) from fluid shifts can lead to decreased tissue perfusion.
Furthermore, hypovolemia can decrease cardiac output.
Less intravascular volume means less venous return to the heart, which can decrease stroke volume and cardiac output.
The combination of the systemic inflammatory response, increased capillary permeability, massive fluid shifts, worsening intravascular hypovolemia, and decreased cardiac output can lead to decreased tissue perfusion.
If not corrected, this can lead to persistent tissue hypoperfusion and/or end-organ damage, a phenomenon known as “burn shock”.
Therefore burn shock is a combination of 3 types of shock:
Distributive Shock (Capillary leak/vasodilation from inflammatory response)
Hypovolemic Shock (Fluid shifts/intravascular fluid depletion)
Cardiogenic Shock (Decreased stroke volume and cardiac output)
The way to manage and/or prevent burn shock from occurring is with aggressive fluid resuscitation.
The goal is to maintain tissue perfusion and prevent end-organ damage by replacing the intravascular fluids that are displaced.
Therefore, fluids play an important role in managing circulation to decrease morbidity and mortality, especially in severe burn patients.
Those with heart failure, kidney disease, or other comorbidities that may affect fluid resuscitation should have their volume status closely monitored.
Burn Shock: A combination of distributive shock from the capillary leak, hypovolemic shock from the intravascular hypovolemia, and cardiogenic shock from the decreased cardiac output can lead to “burn shock”.
Parkland Formula & Others
The importance of fluids should be clear now after reading the above section on the pathophysiology of burns and “burn shock”.
As a result, formulas and protocols exist in order to calculate fluid requirements.
The Parkland formula is one of the most well-known and widely used formulas to calculate initial fluid requirements in severe burn patients.
See above for the Parkland formula and its indications.
While the Parkland formula is popular, there are also other formulas that can calculate the recommended fluid volumes as well.
They include:
Modified Parkland Formula
Brooke Formula
Modified Brooke Formula
Evans Formula
Monafo Formula
Parkland Formula in Pediatrics
Now that we know how to calculate fluid requirements for adults, let’s look at the formula for children.
The formula is the same with the exception of 3mLs instead of 4mLs.
Parkland formula for children:
3mL x Body Weight (kg) x TBSA (%) = Total crystalloid fluids in first 24 hours
Similar to adults, give half this volume over the first 8 hours and the other half over the next 16 hours.
Children should also receive maintenance fluids in addition to their calculated fluid requirements.
The simple way to calculate maintenance fluids in pediatric patients is using the 4-2-1 rule.
Maintenance fluids in children (4-2-1 Rule):
4mL/kg/hr for the first 10 kg of weight plus;
2mL/kg/hr for the next 10 kg of weight plus;
1mL/kg/hr for each kg of weight after 20 kg
Other formulas for children in addition to the Parkland formula include the Shriners Cincinnati and the Galveston formulas.
Parkland Formula for Pediatrics: A child suffering from burns should also receive maintenance fluids in addition to the calculated fluids (which uses 3mLs instead of 4mLs)
Parkland Formula Example: Practice Question
Let’s look at an example to see how the Parkland formula works.
Practice Question
An 80 kg male patient presents with partial thickness burns involving the entire anterior trunk and the entire anterior right arm.
What is the TBSA involved using the Rule of Nines?
How much fluid should the patient receive in the first 24 hours using the Parkland formula?
How much fluid should the patient receive in the first 8 hours? Over the next 16 hours?
Parkland Formula Example and Practice Question
Answer
TBSA = 22.5% (18% anterior trunk + 4.5% anterior right arm)
Total fluids to be given in first 24 hours = 7,200 mL
Total fluids to be given in the first 8 hours = 3,600 mL
Total fluids to be given over the next 16 hours = 3,600 mL
Explanation
First we have to calculate the TBSA involved by the burn.
We will use the Rule of Nines to do this.
We know the anterior trunk has a BSA of 18%, so the partial thickness burns involving the entire anterior trunk have a TBSA of 18%.
There is also a partial thickness burn involving the entire anterior right arm.
We know the entire right arm has a BSA of 9%.
Since this burn only involves the anterior aspect, then TBSA is 4.5%.
Therefore, this patient with partial thickness burns to the anterior trunk and anterior right arm involves a TBSA of 22.5% (18% + 4.5%).
Since the burn is a partial thickness burn and involves more than 20% TBSA, we can use the Parkland formula to calculate the fluid requirements for the first 24 hours.
We know the patient weighs 80 kg and has a TBSA percentage of 22.5, so we will multiple 4mLs x 80 x 22.5.
This will give us 7,200 mLs of fluid recommended within the first 24 hours after burn injury.
Remember half of the total volume (3,600 mL) will be given over the first 8 hours, and the other half of the total volume (3,600 mL) will be given over the next 16 hours.
Parkland formula example and practice question answers
Keep in Mind…
Just a few points to wrap up the Parkland formula.
First, it is important to remember the formulas are guidelines and not hard-and-fast rules.
The Parkland formula may underestimate fluid requirements in some cases, especially inhalation injuries, electrical burns, full thickness burns, etc.
The Parkland formula may also overestimate fluid requirements in other cases.
Under fluid resuscitation can lead to hypotension, poor tissue perfusion, acute kidney injury, end-organ damage, etc.
Over resuscitation can lead to compartment syndromes, acute respiratory distress syndrome (ARDS), etc.
Therefore, you will need to use your clinical judgement and monitor the patient’s fluid status on a case-by-case basis.
For example, you can monitor hourly urine output through a Foley catheter, as well as the patient’s vital signs, respiratory status, and mental status, etc.
After 24 hours of fluid resuscitation, the Parkland formula (and others) will provide you with recommendations for the next 24 hours.
Referenceshttps://www.ncbi.nlm.nih.gov/books/NBK537190/https://www.ebmedicine.net/media_library/files/Burns-Parkland.pdfhttps://www.nursingtimes.net/clinical-archive/accident-and-emergency/parkland-formula-fluid-resuscitation-in-burns-patients-1-using-formulas-03-04-2008/https://pubmed.ncbi.nlm.nih.gov/23448271/https://www.researchgate.net/publication/235755125_The_surface_area_of_the_hand_and_the_palm_for_estimating_percentage_of_total_body_surface_area_Results_of_a_meta-analysishttps://www.uofmhealth.org/health-library/sig254759https://www.theplasticsfella.com/total-body-surface-area-in-burns/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3038406/https://www.msdmanuals.com/en-jp/professional/multimedia/figure/phy_rule_of_nines